
By John Jones, JD PhD, Vaxxter contributor
I am in firm agreement with Jon Rappoport: As news consumers, we’re continually bombarded with sensationalism, encouraging fear, stress, and illness. And all the while, stories of the latest virus, or flu, or “pandemic”, can discourage us from being healthy and understanding how easy it is to be well.
Despite coronavirus talk on the front burner, I have been asked to review the topic of Ebola – which has been bubbling off and on for 40 years in Africa. Though we are told that the epicenter is some far off place, in the Democratic Republic of the Congo (formerly Zaire), a place over 7,500 miles from significant policymakers in the CDC headquarters in Atlanta and the Pentagon in Washington, there are larger issues and more persistent themes implicated. If nothing else, we should focus on maintaining our health through nutrition and hygiene, and remain steadfast in our resolve to resist plans to expand wars into sub-Saharan Africa.
What Are They (not) Saying?
There are three general themes with Ebola news. (1) Ebola is real – be afraid; (2) backward and ignorant savages in Africa cannot be in charge of quelling this global health threat; and (3) wonderful scientists from Europe, Canada, and the United States are battling, day and night, to create life-saving medicines and vaccines … that will be ready … any day now.
And now, for the rest of the story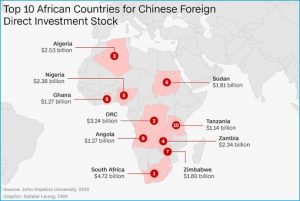
Of course, there is a back story about Ebola in Africa. When considering geopolitical moves, you should know that Africa has an economical and social link to China. China, the world’s number one petroleum importer, is cementing its grip on mining rights, access to African oil, and other resources through mutually beneficial relations that include building roads, railway systems, hospitals, and schools. And some Chinese factories just happen to operate in the Eastern Congo – where Ebola is. Those details aren’t present in the latest chapter of the Ebola Chronicles.
What is Ebola?
According to the WHO (2019),
Ebola virus disease (EVD), formerly known as Ebola hemorrhagic (bleeding) fever, is a rare but often fatal illness in humans. The average EVD case fatality rate is around 50%. Case fatality rates have varied from 25% to 90% in past outbreaks. The virus is transmitted to people from wild animals and spreads … through human-to-human transmission.”
The WHO says that EVD first appeared in 1976 in South Sudan, and Yambuku, Democratic Republic of Congo (DRC). Eastern DRC is the current center for the present outbreak (2018-2019).
Within the same factsheet, agents at the WHO claim that EVD has a unique cause, but the symptoms look oddly familiar. Initial stages of the disease are show as fever, fatigue, headache, and sore throat. As one gets sicker, the symptoms progress to vomiting, diarrhea, rash, impaired kidney and liver function, internal and external bleeding.
Noting that these symptoms are familiar to clinicians and health care providers on the ground in Africa, the WHO (2019) says:
“It can be difficult to distinguish EVD from other infectious diseases such as malaria, typhoid fever, and meningitis.”
This declaration, that Ebola-virus disease presents with nearly the same symptoms as malaria, typhoid, and meningitis should give us a clue about what the allopaths believe – and what approaches they will continue to take. Remember, they claim that Ebola is a deadly disease, supposedly due to virus, that just sprang up – out of nowhere – 40 years ago. And though they have never cured anyone, they are ever ready to try out some new chemical combinations (a patented drug) and or experimental vaccine.
What is Happening on the Ground?
The WHO is sending out press releases, and copy-ready stories announcing that Ebola is a health crisis.
“Since 2018, Ebola virus disease in spreading the eastern Democratic Republic of Congo (DRC). By September 2019, [nearly] 3,000 cases and 2,000 deaths had been reported [by WHO field offices].” Cited in Lucey (2019).
And we are all supposed to understand the reason for the outbreaks and epidemics: locals in the DRC are backward, ignorant, and do not trust science.
According to Hamadou Boiro, the World Health Organization’s social anthropologists team leader, Ebola persists in the northeast of the DRC “because there are some in [the] community who refuse to believe that Ebola exists and refuse to seek treatment.”
Otto (2020) adds some information to assist our appreciation of Congolese people as maniacal, conspiracy theorists:
“In December 2018, a politician told his followers that the disease had been invented by the ruling-Government as an excuse for annulling the presidential vote in the Ebola-stricken areas”; and
“In 2019, WHO recorded around 390 attacks on health care facilities. The attacks killed 11 and injured 83 health workers.”
With such vocal and violent opposition, one might find it easier to leave the Africans to their fate. But recall the lesson from Rahm Emmanuel, ‘you never want a serious crisis go to waste.’

THE BOOT CAMP IS COMING SOON – CLICK HERE FOR MORE INFORMATION
Humanitarian Rescue Efforts or Medical Experiments?
Recently the government of Canada has announced its incursion to help Africans in the Congo. Karina Gould, Minister of International Development, explains that Canada is allocating $45 million CAD. These funds are going to trusted humanitarian partners working in the Democratic Republic of Congo to respond to Ebola-specific and other humanitarian needs. Activities will include providing:
“Health services … logistics and coordination support, such as air services, to improve the… ability to prevent, detect and respond to outbreaks [in the DRC and neighboring countries]; and training for community health workers and immunization campaign.”
And part of Plan Canada will be local PR. According to a January 17 press release from Global Affairs Canada (2020), nearly $1 million CAD will pay for a Peace and Stabilization Operations Program in the region of Nord-Kivu.
“Project activities will include the creation of communications tools to educate communities on Ebola in order to avoid misinformation and myths about the disease.”
But how will people of the Congo and the world learn about Ebola? Should the Africans know that western medicine has never helped?
No Effective Treatment
Writing in the British Medical Journal, Dr. Daniel Lucey (2019) writes:
“Although the first Ebola outbreaks were recognized in DRC and Sudan in 1976, there has never been an effective treatment.” (emphasis added).
According to the WHO factsheet (2019),
(1) Vaccines to protect against Ebola are under development and have been used [sic] to control [sic] the spread of Ebola in Guinea and in the DRC.
(2) Early supportive care with rehydration … improves survival. There is no licensed treatment proven to neutralize the virus but … immunological and drug therapies are under development.
So now we are back to square one.
On the one hand, the WHO tells us that Ebola looks like other viral infections (malaria, typhoid, and meningitis). Viral infections that vaccines and pharmaceutical drugs have overcome [sic].
But we also see glaring admissions that, none of their pseudo-science, mumbo jumbo has ever worked to prevent or cure Ebola. And how could we expect allopathic interventions to heal Ebola infections when those same protocols have not prevented or cured the other three?
Consider, typhoid fever, supposedly caused by the ever-present salmonella typhi bacteria, exploded, starting in the 1800s, in relation to mass smallpox vaccination campaigns. Each year, there are outbreaks of meningitis among vaccinated university students in the United States. Lastly, the Gates Foundation has been telling us, for years, that a malaria vaccine is just around the corner.
Ebola Treatment? Prevent Wellness, but call it a success!
The WHO factsheet from May 2019 offered the following:
“An experimental Ebola vaccine proved highly protective [sic] against EVD in a major trial in Guinea in 2015. The vaccine, rVSV-ZEBOV, was [used] in a trial involving 11,841 people. Among the 5,837 people who received the vaccine, no Ebola cases were recorded, 10 days or more after vaccination. In comparison, there were 23 cases, 10 days or more after vaccination [sic] among those who did not receive the vaccine.”
They add that the rVSV-ZEBOV vaccine is being used in the ongoing Ebola outbreak in DRC that started in 2018.
THE BOOT CAMP IS COMING SOON – CLICK HERE FOR MORE INFORMATION
A Second Look at Merck’s ERVEBO Trial
In December 2016, the Lancet reported on the rVSV-ZEBOV trial from West Africa. The lead author, Ana Maria Henao-Restrepo, and her 31 co-authors working at institutes and universities from the U.S, Canada, South Africa, Belgium, Germany, and the UK declare that the vaccine was 100% effective in preventing Ebola outbreaks.
But … I read the study.
Putting aside their CDC-esque data manipulations, and just looking at the reported data, we see that Henao-Restrepo et al. (2016) and their Merck funders, did not find provide any salvation for poor and malnourished Africans. Once we scratch the surface, we see that:
- some of the vaccinated had acute reactions to the vaccine – arguably worse than Ebola disease itself;
- some of the vaccinated actually fell ill with Ebola, and most significantly,
- for two of the three vaccinated groups, Ebola rates were higher than (i) that of the general population; and (ii) that of other non-vaccinated groups in the study.
Group Division
The trial took people from the nations of Guinea and Sierra Leone. After finding their eligible subjects, the researchers divided them into three categories:
- (A) randomly chosen, and ready to receive the vaccine immediately;
- (B) randomly chosen, and ready to receive the vaccine – but to be injected 21 days later; and
- (C) not randomly chosen, but ready to receive the vaccine immediately.
Groups A and C were further divided into two parts: those who received the vaccine; and those who did not. On the other hand, Group B was whittled down through withdrawn consent, illness, and pregnancy.
Thus, from the perspective of the authors, there were five groups – three of whom received the vaccine, and two who did not. I call the former A1, B, and C1, and the latter A2 and C2. (As 1055 persons initially found eligible to be in Group B were not vaccinated, I will call them B2 and use them for sake of comparison).
Instead of using their terms, we could configure the groups another way: Those who got the vaccine immediately (A1 and C1), those who got the vaccine 21 days after being identified as eligible (B1), and those who were left unvaccinated (what I call Groups A2, B2, and C2).
Lancet (2016) Ebola Vaccine Study: one view of the raw data |
|||||||
| Group A | hGroup B | Group C | Total number | ||||
| Group Name |
(A1) vaccinated |
(A2) non- vaccinated | (B1) vaccine delayed | (B2) non- vaccinated | (C1) vaccinated | (C2) non- vaccinated | |
| Number of subjects | 2119 | 1113 | 2041 | 1055 | 1667 | 329 | 8026 |
| Ebola (+) cases | 11 | 16 | 16 | 21 | 10 | 1 | 75 |
| Ebola cases per 10,000 | 52 | 81 | 19.6 | 68 | 60 | 30.4 |
60.2 |
The results of this study tell us a few things.
Aside from fact that the vaccine had negligible effects (see more below), for the nations of Guinea and Liberia, Ebola was not a significant health problem. By contrast, in Guinea, death rates from malaria and respiratory infection are over 16 times greater than what Ebola was – at its peak. Similarly, there are 7 times more deaths prevalent to Ebola in comparison to combining deaths of TB and meningitis.
Why Would the Vaccine Fail?
Despite the real numbers – present in their own study, the researchers state that ERVEBO was 100% effective against Ebola (Henao-Restrepo et al. 2016). That is, if ANYONE receives a shot, early enough and before exposure, the vaccinee will never get Ebola.
But there are reasons why the rVSV- ZEBOV vaccine cannot improve health. And these facts were published before the experimental vaccine was injected into unwitting Africans of Guinea and Liberia.
As we know, modern medicine determines the efficacy of a vaccine based on the production of antibodies. (See Plotkin 2010). But it turns out, that in relation to VSV (vesicular stomatitis virus, aka mouth ulcer virus), antibodies per se, and those stimulated by VSV vaccines are not necessary for immunity! (See Moseman et al. 2012).
Hence, Merck’s package insert for ERVEBO reads:
14.2 Clinical Immunogenicity:
A measure of the immune response that confers protection against EVD is unknown. (emphasis added)
Yes, you read it correctly, even Merck says that they have no idea if the vaccine confers protection against Ebola disease.
Useless Injections
The lack of understanding between a recombinant VSV vaccine, like ERVEBO, any antibodies produced post injection, and the prevention of EVD is evidenced from the study of Qiu et al. (2009). That team used a recombinant virus, made up of VSV and Ebola proteins, on macaque monkeys. Though the animals survived a high dose of injected Ebola virus, over the course of 28 days, there was effectively no reduction in the amount of Ebola virus in their blood. (See figure 3 in Qiu et al. 2009). The study also lacked adequate size and a reasonable length of time. The researchers only injected two macaques with the vaccine (n = 2), and similarly, the control group was only two monkeys (n = 2). And though the vaccine group lived 28 days, Qiu et al. (2009) euthanized the control group after a mere six days.
Noting the low rate of Ebola infection, even in impoverished and malnourished populations, and the lack of evidence that any vaccine provides a benefit, is a vaccine needed? The simple answer is, “No.” According to a CNN editorial of 2014 (updated in December of 2019):
“Ebola is extremely infectious, but not extremely contagious.” (emphasis added).
Little surprise then, in relation to the Ebola reports starting in 2013, even though there was and is no drug therapy, and no proven vaccine – and no shots were ever given to the entire at-risk population in West Africa, by 9 June 2016, WHO representatives declared that Liberia was Ebola-free.
Somehow a pathogen, causing infection, illness, and death, just went away.
Giving Africans Experimental Drugs
There are two experimental trial reports for the people in the Congo. One by Amy Maxmen (2019) writing for Nature magazine, the other is printed in the New England Journal of Medicine (12 December 2019). Because the numbers vary slightly, I will use the figures from the academics (Mulangu et al. 2019) as published in the NEJM.
People were assigned into four groups and either injected with antibody cocktails (biologics) or given antiviral pills to ingest. Guess what happened? They died – but the drug makers, and Nature magazine, and the editors at the NEJM, called it a success!
| Treatment (drugs) | MAb114 | REGN-EB3 | ZMapp | Remdesivir |
| number | 174 | 155 | 169 | 175 |
| deaths by day 28 | 61 | 52 | 84 | 93 |
| death rate % | 35.1 | 33.5 | 49.7 | 53.1 |
| Source: Mulangu et al. (2019): Table 2 | ||||
Death by Experimentation
As noted above, the WHO says that the fatality rate for an Ebola infection ranges from 25-90%, with an average of about 50%. An unattributed line on a Wikipedia site claims that the death rate is around 70%. But clearly, none of the treatment protocols reached survival rates over 68%. Rather, each of the four groups experienced death rates within the expected range – for people receiving no treatment.
Importantly, the experiment saw 290 of 673 people die within four weeks of being helped by these agents of war, profit and social control. The project was mostly funded by the United States government – NIAID, NIH, HHS, our friends at the WHO, and the drugmakers. The US Department of Defense provided the MAb114, Gilead gave the remdesiver, Mapp provided the ZMapp, Regeneron asked the team to test its latest, REGN-EB3.
And in case you were worried about the integrity of the science, Mulangu et al. (2019) added a caveat:
“Twelve patients were enrolled, but died before receiving the first infusion: one in the ZMapp group, three in the remdesivir group, three in the MAb114 group, and five in the REGN-EB3 group.”
Treatment With Antiviral Drugs?
Why these four drugs specifically for this study? Though REGN-EB3, MAb114, and ZMapp are antibody therapies, remdesivir is a so-called anti-viral. According to Anthony Fauci, Director of the U.S. National Institute of Allergy and Infectious Diseases (NIAID), his department has been working with Gilead closely to test whether remdesivir, a drug that could also be used for people diagnosed with coronavirus.
What is Remdesivir?
Remdesivir is a combination of carbon, hydrogen, nitrogen, oxygen, and phosphorous. Its chemical formula is C27H35N6O8P. In this respect, it is similar in its structure to essential phospholipids including phosphatidylserine, phosphatidylcholine, and phosphatidylethanolamine. These phospholipids play a vital role in protecting cell integrity – keeping out foreign proteins and other toxins (e.g., heavy metals). When we see people fall ill with Ebola, a hemorrhagic fever, we see internal bleeding, indicative of a loss of cellular integrity.
Additionally, remdesivir is similar to ATP (adenosine triphosphate) which has a chemical structure of C10H16N5O13P3. So it is likely that a person taking remdesivir could experience a short-term benefit, but it does not and cannot provide the amount of phosphorous and other significant elements that the body requires.
Back to Basics: It’s the nutrition, stupid!
Over the last 40 years, I have researched health and nutrition. Thanks to the internet, I have learned from the likes of Dr. Sherri Tenpenny, Dr. Suzanne Humphries, Dr. John Bergman, Dr. Sherry Rogers, Robert Scott Bell, Gary Null, and Joel Wallach. We do not worry about Ebola, or coronavirus, or flu, or HPV, or Hepatitis, or measles, polio, or pertussis, or any other germs. Nor are we shocked nor alarmed that two or three times a year, the WHO, CDC, or others announce a new outbreak. We know that health is from the inside out – it starts with nutrition and includes personal and public hygiene.
Undoubtedly, people diagnosed as being ill with Ebola infection, are suffering from scurvy, extreme Vitamin C deficiency. Like those with scurvy, severe Ebola illness is characterized by capillary fragility, and a tendency to bleed easily.
Vitamin C For Boosting
Thomas Levy, MD, JD, has researched the applications of vitamin C. From his book Vitamin C, Infectious Diseases, and Toxins: Curing the Incurable, he includes a reference:
“Cathcart (1981), who introduced the concept of bowel tolerance to vitamin C … hypothesized that Ebola, like other acute viral hemorrhagic fevers, might well require 500,000 mg of vitamin C daily to reach bowel tolerance … oral administration should begin simultaneously, but the intravenous route should not be abandoned [until the patient has recovered]. As death can occur quickly with the hemorrhagic fevers, one cannot be conservative when dosing the vitamin C.”
In addition to vitamin C and the essential fatty acids, the immune function can be boosted with vitamin D3, selenium, and zinc. Selenium is extremely critical for the people of the eastern Congo because the soils there are depleted in selenium.
Has anyone from the WHO or even the local health officials in Congo, Liberia, Guinea turned to nutrition and food as a basic therapy?
They never will.
But when told of the next impending virus, what will you do?
++++++++++++++++++++++++++++++++
 Like what you’re reading on Vaxxter.com?
Like what you’re reading on Vaxxter.com?
Share this article with your friends. Help us grow.
Join our list here or text MVI to 555888
+++++++++++++++++++++++++++++++++++++
John C. Jones received his law degree (2001) and his Ph.D. is in political science (2003) from the University of Iowa. He has over 15 years of research and writing (both academic and journalistic) in fields of public policy and law, criminal and Constitutional law, and philosophy of science and medicine. His additional areas of expertise and specialized knowledge include applied statistics, etymology, political communications/public relations, litigation and court procedure. He has a particular interest in the science and history of vaccines.
Photo credit: ID 47415316 © Macgyverhh | Dreamstime.com